 The site of a beating heart glistening and pumping is like no other site I have ever seen. The heart is simply amazing. It's more than just a four-chambered pump; it is well-designed machine that keeps our blood flowing to our muscles and lungs, ensuring we receive oxygen and nutrients to sustain ourselves.
The site of a beating heart glistening and pumping is like no other site I have ever seen. The heart is simply amazing. It's more than just a four-chambered pump; it is well-designed machine that keeps our blood flowing to our muscles and lungs, ensuring we receive oxygen and nutrients to sustain ourselves.But when the heart becomes damaged, we compromise our ability to circulate our blood to our tissues. This is a bad thing. And sometimes, we must intervene to repair this amazing machine.
When I walked into the OR with Dr. N, an anesthesiologist, I was awe-stricken. There was the heart sitting snugly in the middle of the chest, completely exposed.
To gain access to the heart, the chest literally had to be cracked along the sternum. The middle flaps of skin, fat, and muscle were pulled to the side, opened with large scoop-like metal instruments. The result was a square window, where the heart was exposed, and the surgeons were busily working to the tune of the ECG and Blood monitor beeps.
I gained an interesting vantage point; I stood from behind the blue drape that covers the patient's face. From above the blue, I could see the red blood and heart. And behind me, the monitors beeped, flashed numbers, showed squiggly lines--revealing the overall state of the heart through each stage of the surgery.
Watching the surgeons work around the heart took me back to anatomy. I can still remember the day in anatomy lab, when we each passed the scalpel around to cut the heart out of our cadever. When I held the heart in my hand, I could only think- "this was some one's heart- wow!"
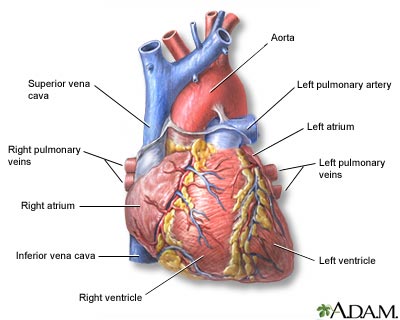
Performing an invasive open heart surgery is long and complicated. The surgeon's were performing a mitral valve replacement. Essentially, the valve that separates the left atria from the left ventricles in our patent's heart was no longer functioning properly. If left untreated, a broken valve can lead to heart failure or severe cardiac complications. So, surgical intervention is necessary.
To place a new valve into the heart, the heart has to stop beating and must be kept cold (to protect the heart). While the heart stops beating, the blood is pumped out of the body through a cardiopulmonary bypass machine, which adds oxygen. So, the machine effectively acts as the heart, while the real heart is being repaired.
The surgeon's gloved hands skillfully sutured the new valve into the heart, as well as other areas of the heart that had be cut earlier in the procedure. And when the heart was ready, it had be be shocked to start pumping again.
I left the OR at 5 PM. By then, the surgery that had started earlier that morning was still underway. Metal wires were loosely placed through the two sides of the opened chest. The heart was being closely monitored, suction was used to remove any remaining blood, the last sutures were being placed, and the heart was pumping with full force.
**Image: "Open Heart Surgery." http://images.jupiterimages.com/common/detail/46/71/23127146.jpg

.JPG)

















{kind=link}
{kind=link}