
"Musa, what is your New Year's resolution?"
"Let's see, number 1- do not tell others my resolutions." Musa is a smart kid.
It's hard to believe that 2007 will end in a matter of hours and we will soon ring 2008. With the New Year also comes the deluge of resolutions. There is also the challenge of reprogramming our pens/pencils/brains that it is 2008.
***Note to self: remember to write 2008.
As we bring in the New Year, we take with us memories of 2007 and hope that 2008 will be even more amazing (at least this is my wish). I really can not complain. 2007 has been unforgettable.
I graduated from college, started medical school, moved to SF, and started my new life as a medical student. Most importantly, I have been so lucky to be surrounded by my family and some wonderful friends, old and new.
I have no idea what 2008 will bring.
In the Spirit of the New Year's I will lay out my resolutions in a nicely organized list for my reference. By no means do I expect my resolutions to dictate my life; it will just offer some guidance.
Ok, here goes (in no special order):
1. Spend more time with family and friends.
*There will always be an endless list of "stuff to do" (as demonstrated by this resolution list), but as I get older I am realizing the importance of the individuals who make the moments of my life memorable and meaningful.
2. Discover and better define my spiritual self
*Let's leave at this. This is an evolving and personal quest requiring lots of introspection and inquiry.
3. Maintain a balanced life
*As a medical student, it is so easy to get bogged down by the details, stress, and studying. But as the old saying goes: "work hard and play hard." Life is always a balancing act and it is time to learn how to gracefully do this.
4. Stay Healthy
*As a future physician, I would like to be an example so that I can truly practice what I preach. So, this year I aim to eat 5 servings of vegetables and fruit per day and excercise every day. This will be difficult. But honestly, I exercise to live and I live to eat. I would like diversify my workouts, spend more time outdoors, and one-day run a marathon. I will start by training for a 10K or...5K. Baby steps.
5. Explore SF
*Everyday I feel so lucky to be surrounded by a city that is bustling with life and culture. I have yet to imbibe the essence of the city. I'll start with more regular runs through Golden Gate Park (see how I can multi-task and accomplish goal 4 and 5).
6. Give back to the community
*I look forward to teaching elementary school students about science and continuing my work at the student-run free clinics in SF and Sacramento. I hope I can incorporate my photography into service work and find new ways to impact the lives of others. Any ideas?
7. Be more creative
*Spend more time behind the lens of my camera and writing about anything and everything.
8. Become informed about current events and health care issues
9. Solve the health care crisis
*Ok, this is highly ambitious. But I'd like to be involved somehow.
10. Learn outside the box
*Lectures and textbooks can only teach me so much. There has to be a more effective way to retain information.
11. Master languages: Punjabi, Urdu, and Spanish
12. Cook more and cook for the people I like
13. Learn more about my classmates and their stories
14. Travel somewhere outside California (and possibly outside the United States)
15. Figure out what "kind" of doctor I want to be so that I can give a response to every person that asks me what "kind of doctor I want to be."
16. Enjoy Life. Stay Happy. Stay Calm. Stay Free.
Happy New Year's everyone. I look forward to celebrating the first few moments of 2008 with my dearest friends. Best wishes with your resolutions and enjoy the last hours of 2007.
Cheers!
"Let's see, number 1- do not tell others my resolutions." Musa is a smart kid.
It's hard to believe that 2007 will end in a matter of hours and we will soon ring 2008. With the New Year also comes the deluge of resolutions. There is also the challenge of reprogramming our pens/pencils/brains that it is 2008.
***Note to self: remember to write 2008.
As we bring in the New Year, we take with us memories of 2007 and hope that 2008 will be even more amazing (at least this is my wish). I really can not complain. 2007 has been unforgettable.
I graduated from college, started medical school, moved to SF, and started my new life as a medical student. Most importantly, I have been so lucky to be surrounded by my family and some wonderful friends, old and new.
I have no idea what 2008 will bring.
In the Spirit of the New Year's I will lay out my resolutions in a nicely organized list for my reference. By no means do I expect my resolutions to dictate my life; it will just offer some guidance.
Ok, here goes (in no special order):
1. Spend more time with family and friends.
*There will always be an endless list of "stuff to do" (as demonstrated by this resolution list), but as I get older I am realizing the importance of the individuals who make the moments of my life memorable and meaningful.
2. Discover and better define my spiritual self
*Let's leave at this. This is an evolving and personal quest requiring lots of introspection and inquiry.
3. Maintain a balanced life
*As a medical student, it is so easy to get bogged down by the details, stress, and studying. But as the old saying goes: "work hard and play hard." Life is always a balancing act and it is time to learn how to gracefully do this.
4. Stay Healthy
*As a future physician, I would like to be an example so that I can truly practice what I preach. So, this year I aim to eat 5 servings of vegetables and fruit per day and excercise every day. This will be difficult. But honestly, I exercise to live and I live to eat. I would like diversify my workouts, spend more time outdoors, and one-day run a marathon. I will start by training for a 10K or...5K. Baby steps.
5. Explore SF
*Everyday I feel so lucky to be surrounded by a city that is bustling with life and culture. I have yet to imbibe the essence of the city. I'll start with more regular runs through Golden Gate Park (see how I can multi-task and accomplish goal 4 and 5).
6. Give back to the community
*I look forward to teaching elementary school students about science and continuing my work at the student-run free clinics in SF and Sacramento. I hope I can incorporate my photography into service work and find new ways to impact the lives of others. Any ideas?
7. Be more creative
*Spend more time behind the lens of my camera and writing about anything and everything.
8. Become informed about current events and health care issues
9. Solve the health care crisis
*Ok, this is highly ambitious. But I'd like to be involved somehow.
10. Learn outside the box
*Lectures and textbooks can only teach me so much. There has to be a more effective way to retain information.
11. Master languages: Punjabi, Urdu, and Spanish
12. Cook more and cook for the people I like
13. Learn more about my classmates and their stories
14. Travel somewhere outside California (and possibly outside the United States)
15. Figure out what "kind" of doctor I want to be so that I can give a response to every person that asks me what "kind of doctor I want to be."
16. Enjoy Life. Stay Happy. Stay Calm. Stay Free.
Happy New Year's everyone. I look forward to celebrating the first few moments of 2008 with my dearest friends. Best wishes with your resolutions and enjoy the last hours of 2007.
Cheers!
***










.jpg)







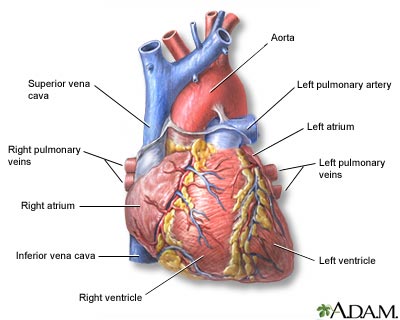
 The site of a beating heart glistening and pumping is like no other site I have ever seen. The heart is simply amazing. It's more than just a four-chambered pump; it is well-designed machine that keeps our blood flowing to our muscles and lungs, ensuring we receive oxygen and nutrients to sustain ourselves.
The site of a beating heart glistening and pumping is like no other site I have ever seen. The heart is simply amazing. It's more than just a four-chambered pump; it is well-designed machine that keeps our blood flowing to our muscles and lungs, ensuring we receive oxygen and nutrients to sustain ourselves.
.JPG)
















{kind=link}